
History and Background
Since ACL and CMS began funding Aging and Disability Resource Center (ADRC) development in 2003, ADRCs have been working to assist individuals in critical pathways, defined as times or places where people make important decisions about long-term care. This work has included several innovative interventions to facilitate the hospital discharge process and to help nursing facility residents return to the community.
The 2009 ACL program announcement for ADRCs, “Empowering Individuals to Navigate Their Health and Long-Term Support Options,” emphasized reaching people during transitions from one care setting to another, identifying person-centered hospital discharge planning as a key operational component.
In 2010, the Patient Protection and Affordable Care Act (ACA) provided $50 million over five years to support further development of the ADRC Program such as the ADRC Evidence Based Care Transitions Program. In addition, the ACA funded the CMS Balancing Incentive Program to incentivize states to rebalance Medicaid Long-term Services and Supports (LTSS) spending, and required participating states to make changes to their LTSS systems, including developing a statewide No Wrong Door (NWD) System. Many state Medicaid agencies included ADRCs in the development of their Balancing Incentive Program NWD System.
Recognizing the accomplishments of the ADRC and Balancing Incentive Programs, as well as lessons learned from the experience of states participating in these and other LTSS initiatives, ACL, CMS, and the Veterans Health Administration (VHA) issued a funding announcement: the 2012 “Part A: The Enhanced ADRC Options Counseling Program.” It reflected the key lessons learned to date, including the realization that no single agency or network can successfully implement a LTSS access system for all populations and all payers without multiple agencies and organizations at the state and local level formally involved in the system's operations. Many agencies and organizations that serve or represent the interests of different LTSS populations must be involved. The new FOA embraced this lesson by officially adopting the NWD model.
- Purpose of the Program
-
The 2010 ADRC Evidence Based Care Transitions program supports state efforts to significantly strengthen the role of ADRCs in implementing evidence-based care transition models that meaningfully engage older adults and individuals with disabilities (and their informal caregivers). This grant program was designed to promote the further development and enhancement of ADRC participation in evidence-based care transition models. This includes:
- Expanding the reach of the ADRC efforts (e.g., training staff, adding additional staff, expanding an intervention to serve new populations, or expanding to additional sites).
- Strengthening the extent to which existing transitions programs operated by hospital and health systems leverage the assets of the ADRCs (e.g., to streamline access to public benefits, link individuals with community-based services and supports, and counsel individuals and their families on service options) where ADRCs currently have a limited role.
- Informing ACL/CMS, other federal agencies, and Congress on national policy related to care transitions, hospital discharge planning, person-centered planning, and mechanisms to reduce unnecessary hospital re-admissions.
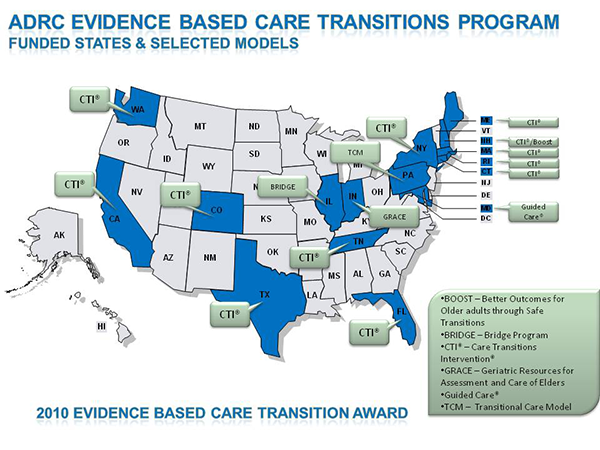
The six evidence-based care transition models implemented by grantees included:
- Better Outcomes for Older adults through Safe Transitions (BOOST)
- Bridge program
- Care Transitions Intervention®
- Geriatric Resources for Assessment and Care of Elders (GRACE)
- Guided Care®
- Transitional Care Model
In 2010, ACL issued awards to 16 states implementing six evidence based care transition models. Select a state below for its project summary.
- California (PDF, 27KB)
- Colorado (PDF, 26KB)
- Connecticut (PDF, 27KB)
- Florida (PDF, 26KB)
- Illinois (PDF, 16KB)
- Indiana (PDF, 16KB)
- Maine (PDF, 31KB)
- Maryland (PDF, 16KB)
- Massachusetts (PDF, 27KB)
- New Hampshire (PDF, 27KB)
- New York (PDF, 27KB)
- Pennsylvania (PDF, 18KB)
- Rhode Island (PDF, 27KB)
- Tennessee (PDF, 26KB)
- Texas (PDF, 26KB)
- Washington (PDF, 26KB)
- ADRC Evidence Based Care Transitions Program
-
The 2010 ADRC Evidence Based Care Transitions Program Announcement also included a special funding opportunity made available by The Center for Technology and Aging, with support from the SCAN Foundation, to support the use of assistive technologies in the Evidence-Based Care Transitions Programs funded through this program.
Key program results to date include:
- 22 ADRCs are partnering with 67 hospitals in 16 states
- 20 ADRCs have supported the transition of 7,530 consumers
- 16 ADRCs are partnering with Quality Improvement Organizations (QIOs)
- ADRCs are also partnering with a myriad of other organizations, including:
- Alzheimer’s Association Local Chapters
- Accountable Care Organizations
- Beacon Communities
- Community Health Centers
- Food Pantries
- Health Care Facilities Associations
- Health Homes
- Health Information Exchanges
- Home Health Agencies
- Homeless Shelters
- Hospital Associations
- Hospital Engagement Networks (HENs)
- Housing Organizations
- Human Rights Agencies
- Local Health Councils
- Managed Care Organizations
- Mental Health/Substance Abuse Providers
- Patience Centered Medical Homes
- Pharmacies and Pharmacy Associations
- Physician Medical Organizations
- Primary Care Providers
- Protective Services
- Public Health Departments
- Quality Improvement Organizations
- Rural Health Networks
- State Health Insurance Programs
- Skilled Nursing Facilities
- Universities
- Volunteer Organizations
For more information, please contact Caroline Ryan at caroline.ryan@acl.hhs.gov.
- Care Transitions and a State’s No Wrong Door System of Access to LTSS
-
A key function of the No Wrong Door (NWD) System is to serve as a bridge for the health system to the community and to facilitate the transition of individuals with LTSS needs who are being discharged from acute care settings back to their own homes. The NWD System also helps these individuals to arrange for the community services and supports they need to remain at home and avoid unnecessary hospital re-admissions. The state helps ensure that a subset of NWD staff doing Person-Centered Counseling have the experience and skills required to successfully transition individuals from acute care settings back to the home. The state also ensures that NWD organizations with this expertise have formal agreements with acute care entities that define the role of the NWD staff in facilitating hospital-to-home transitions for people with LTSS needs.
As a result of ACL investments in local ADRC care transitions activities, ADRCs across the country are serving as a resource for acute, primary and related health professionals and provide the healthcare system with a community-based services and supports. ACL is building upon ADRC evidence based care transition experience through the No Wrong Door System. Quick connections to LTSS also break the cycle of avoidable hospital re-admissions and improve individual outcomes in the community and quality of life.
- Care Transitions Resources
-
For Administrators
- Centers for Medicare and Medicaid Services: Community-based Care Transitions Program
The Community Based Care Transitions Program (CCTP) goals are to reduce hospital re-admissions, test sustainable funding streams for care transition services, maintain or improve quality of care, and document measurable savings to the Medicare program. The demonstration will be conducted under the authority of section 3026 of the Affordable Care Act of 2010. - AHRQ Health Care Innovations Exchange
This Exchange helps to solve problems, improve health care quality, and reduce disparities. - Center for Medicare and Medicaid Innovation
This Center is a new engine for revitalizing and sustaining the Medicare, Medicaid, and CHIP programs and ultimately to help to improve the healthcare system for all Americans. Established by the ACA, the Center was given the flexibility and resources to rapidly test innovative care and payment models and scale up successful models.
For Individuals and Families
Planning Ahead
- AHRQ Patient Safety Network
Taking Charge of Your Healthcare: Your Path to Being an Empowered Patient
This toolkit includes comprehensive information for patients and families to facilitate safe transitions from hospital to follow-up care. - Ask Medicare: Tips and Resources for Caregivers
Preparing for Discharge
- Your Discharge Planning Checklist: For patients and their caregivers preparing to leave a hospital, nursing home, or other health care setting (PDF)
This checklist includes important things you and your caregiver should know to prepare for discharge. - Taking Care of Myself: A Guide for When I Leave the Hospital
This guide for patients can help them to care for themselves when they leave the hospital.
- Centers for Medicare and Medicaid Services: Community-based Care Transitions Program